국내 성인의 신체활동 증진을 위한 모바일 헬스 개입: 건강 형평성 중심의 체계적 검토
Abstract
Objectives
This study systematically review the existing literatures to identify the effectiveness of physical activity promotion programs using mobile health (mHealth) among Korean adults, with a focus on factors affecting health equity.
Methods
To search for studies published in the past 10 years (from January 2013 to April 2023), Korean DBs (KoreaMed, KMBASE, KISS, RISS) were used. Hedge'g values were calculated to present uniform quantitative effect estimates for each study and to present pooled effect sizes for the same variables. Additionally, GRADE was used to assess the certainty of evidence and the review was conducted using the PROGRESS-Plus framework for health equity review.
Results
Of the 1,204 literatures, 15 literatures were selected. Six prevention-based mHealth interventions and nine management-based mHealth interventions had significant effect sizes on multiple physical activity-related variables. A review of the PROGRESS-Plus factors revealed that personal characteristics (age, illness), occupation, and gender were the most frequently considered factors affecting health equity, while race, ethnicity, culture, language, religion, features of relationships, and time-dependent relationships were not considered.
Conclusions
The results of the current study confirm the potential of mHealth-enabled physical activity promotion interventions to manage health and prevent disease in Korean adults. It also highlights the need to consider health equity in all phases of research design, implementation, and evaluation to provide opportunities for inclusive participation of a broad range of populations.
Key words: Health equity, Mobile health, Exercise, Systematic review, Republic of Korea
서 론
현대사회는 과학기술의 발달로 편리한 생활을 하고 있지만, 좌식 생활양식이 증가함에 따라 신체활동 부족과 그에 따른 질병의 증가가 사회적 문제로 대두되고 있다[ 1]. 신체활동은 심폐기능 및 근기능을 개선하고[ 2], 만성질환 유병률 저하[ 3], 정신건강기능 향상[ 4] 등의 이점이 있다. 하지만 국민건강영양조사를 통해 확인된 19세 이상 성인의 유산소 신체활동 실천율은 2016년 47.8%, 2018년 44.9%로 지속 감소하는 추세이며, 근력 신체활동 실천율도 2016년 20.7%, 2018년 22.3%로 국민건강증진종합계획 2020의 목표치인 22.8%에 미치지 못하는 수준으로 확인되었다[ 5]. 최근 시장이 확대되고 있는 디지털과 헬스케어를 연계한 모바일 헬스(mHealth) 서비스는 신체활동 실천율 저하의 원인을 해결하는 새로운 방안으로 주목받고 있다. mHealth는 스마트폰, 환자 모니터링 장치 등과 같은 모바일 장치가 지원하는 의료 및 공중 보건 서비스를 의미하며[ 1], 건강관리 서비스 적용범위 확대 및 건강관리의 질 향상과 동시에 시공간, 경제적 제약 없이 누구나 서비스 이용을 가능하게 한다[ 6]. 또한 일상생활과 밀접하게 결합된 스마트폰을 활용하여 지속적인 프로그램 참여 및 운영이 가능하고[ 7], 신체활동 영역에서 스마트폰을 활용하여 실시간 모니터링과 피드백을 제공하는 자가관리 방식의 서비스가 신체활동 및 건강관리에 긍정적 효과가 있음이 확인되었다 [ 8- 10]. 따라서 mHealth 서비스를 활용한 신체활동 증진 서비스 제공시 프로그램 참여를 통한 지속적인 자가관리의 이점을 기대할 수 있으며, 스마트폰을 활용한 서비스로 대상자의 접근이 쉬워진다는 장점이 있다. mHealth를 통해 건강관리 서비스 이용의 장벽을 낮추는 것은 건강 형평성 측면을 고려한 접근으로, 국내에서는 건강 형평성 제고를 위한 노력으로 국민건강증진법의 개정을 통해 건강 취약집단에 대한 지원 방안이 국민건강증진종합계획에 포함되도록 법제화한 바있다. 이에 따라 국내의 건강관리 정책 수립의 로드맵인 국민건강증진종합계획에 ‘건강 형평성 제고’가 제2차(National Health Plan 2010, ‘06-’10)부터 총괄 목표로 추가되었다[ 11]. 하지만 한국은 소득불평등도가 경제협력개발기구(Organisation for Economic Co-operation and Development, OECD) 국가 중 7번째로 높으며, 특히 기업규모에 따른 생산성 격차로 소득 및 사회적 보호의 격차, 고령층의 퇴직 후 소득감소로 인해 소득 양극화가 악화되고 있다[ 12]. 또한 국민건강증진종합계획 2020의 결과를 통해 소득, 지역에 따른 건강 형평성 현황을 검토한 결과 22개의 세부 지표 중 59.1%에 달하는 13개의 지표에서 격차가 증가한 것으로 확인되었다[ 13]. 따라서 건강관리 서비스는 설계부터 개발 및 운영 시까지 형평성에 대한 고려가 필요하지만, 형평성을 중심으로 신체활동 증진 연구 현황을 체계적으로 분석한 국내 연구는 찾아보기 어렵다. 따라서 본 연구에서는 최근 10년간 모바일 헬스 서비스를 활용하여 신체활동 증진 중재 프로그램을 개발·적용한 성인 대상 국내 연구의 효과를 검토하고, 형평성 검토를 위한 프레임워크인 PROGRESS-Plus를 적용하여 건강 형평성 중심의 체계적 문헌고찰을 시행하고자 한다.
연구 방법
연구설계
본 연구는 국내 성인을 대상으로 신체활동 증진을 위해 시도한 예방 및 관리기반 mHealth 중재의 효과와 건강 형평성 중심의 검토를 시행한 체계적 문헌고찰 연구이다.
문헌검색 및 선정기준과 배제기준
본 연구의 문헌분석 과정은 Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA)과 한국보건의료연구원의 체계적 문헌고찰 메뉴얼에 따라 수행되었으며[ 14, 15], 검색프로토콜은 PROS-PERO에 등록되었다(RD42022347841). 최초 문헌검색은 2022년 12월 25일부터 31일까지 실시하였고, 새로 게시된 문헌을 포함하기 위해 2023년 4월에 검색을 반복하였다. 국내 학술지 논문과 국내 학위논문을 검색하였으며, 학위논문이 학술지에 출판된 경우 학술지에 게재된 논문을 선택하였다. 검색은 한국보건의료연구원에서 권장하는 COre database 중 KoreaMed, KMBASE, KISS와 RISS 검색원을 포함하여 수행하였다. 검색어는 신체활동, 운동, 어플리케이션의 유사 및 관련 용어를 결합하였다. 문헌검색은 연구자 1인이 모든 검색원에 대한 검색을 독립적으로 시행한 후, 다른 연구자 1인이 동일 검색어를 활용하여 재검색을 시행하고 검색된 문헌이 일치하는지 확인하였다. 본 연구의 연구대상(P)은 국내 거주 성인이며 단일 질환 환자를 대상으로 한 연구는 제외하였다. 중재(I)는 신체활동 증진을 시도한 mHealth 개입이며, 신체활동을 포함한 mHealth 중재를 시행하였으나, 신체활동과 관련된 결과를 보고하지 않은 연구는 제외하였다. 비교중재(C)는 mHealth 이외 신체활동 중재를 시도하거나, mHealth 서비스를 활용하여 모니터링만 시행한 경우, 특이 중재 없이 일상생활을 시행한 중재이다. 결과(O)는 신체 활동량을 측정하는 객관적 지표(걸음수, 운동 이행 횟수 등)나 신체활동과 직·간접적 관련성을 지닌 도구로 수집된 결과(운동 자기효능감, 운동 결과기대, 운동순응도, 운동 만족, 신체 활동량 등), 신체활동으로 변화가능한 신체계측 결과(체중, 허리둘레, 악력, 혈압, 채질량지수, 허리둘레와 엉덩이둘레의 비율 등), 검사실 검사결과(fasting blood sugar, total cholesterol, triglyceride 등) 중 적어도 하나 이상의 결과를 평균, 표준편차, 대상자 수로 보고한 연구이다. 연구설계는 randomised controlled trials (RCT) 및 quasi-experimental study를 포함하였으며, quasi-experimental study에서 단일군 비교연구는 제외하였고, 최근 10년 이내 발표된 논문을 포함하였다.
분석문헌 선택 과정
검색된 논문은 두 명의 연구자에 의해 독립적으로 검토되었다. 국내 데이터베이스에서 문헌검색 시행 후 이중문헌을 제외하고, 논문의 제목과 초록을 검토하여 선정기준을 검토하였고, 마지막으로 원문을 검토하여 문헌을 선정하였다. 검색된 논문은 체계적 문헌 고찰을 위한 온라인 관리 프로그램인 Covidence와 Endnote, Excel을 이용하여 정리 하였다. 최초 검색을 통해 총 1,204개의 논문이 검색되었고, 검색을 통해 확인된 논문의 참고문헌을 통해 5개의 논문이 추가로 선정되었으며, 검토과정을 통해 최종 선정된 논문은 15편이었다( Figure 1). 그중 Han [ 16]과 An and Lee [ 17]의 연구는 두 개의 실험군(a, b)을 사용하여 설계된 연구였다.
Figure 1.
PRISMA flow for study. PRISMA, preferred reporting items for systematic reviews and meta-analysis. 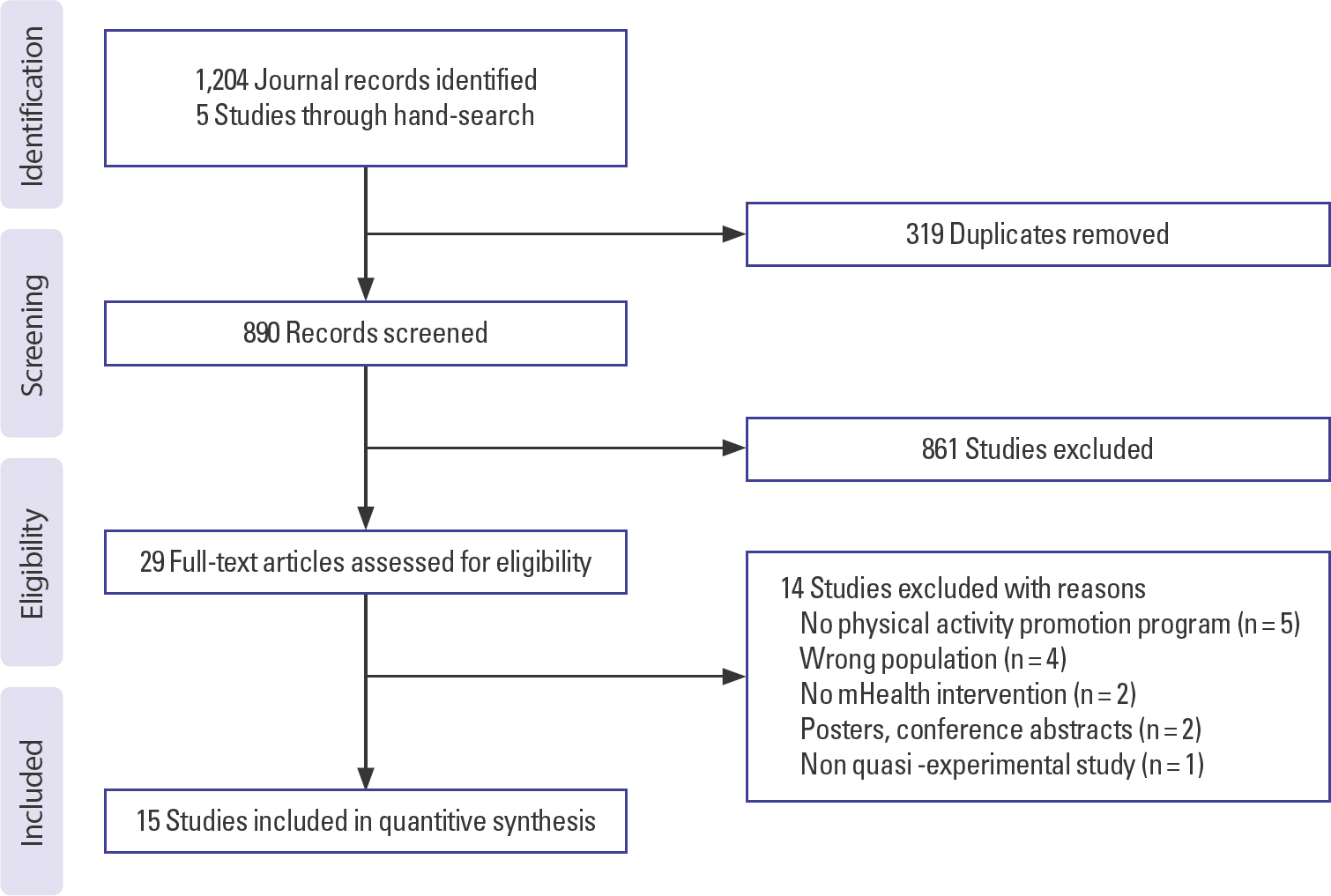
문헌의 질평가
문헌의 질평가는 RCT는 Risk of bias (RoB), quasi-experimental study 는 Risk of Bias In Non-randomized Study of Interventions (ROBINS-I) 도구를 사용하여 수행하였다. 검토자 중 한 명이 각 연구에 대한 평가를 수행한 후 두 번째 검토자가 이를 확인하였다. 불일치에 대해서는 토론과 합의로 해결되었으며, 본 과정을 통해 제외된 연구는 없었다.
자료분석
• 데이터 수집양식을 활용하여 논문의 특성(저자, 년도, mHealth의 형태, 대상자 수, 대상자, 중재 기간, 중재, 대조군, 연구설계, 질평가 결과, 논문출처)을 추출하였다. • 포함된 연구를 신체활동 증진 중재의 특성에 따라 예방기반, 관리기반으로 분류하고, 각 연구에 대해 균일한 정량적 효과 추정치를 제시하기 위해 Hedges’ g 값을 산출하였다. 연구의 결과 중 연구간 동일한 결과에 대해서는 통합된 효과 추정치를 산출하였다. Hedges’ g 값은 중재 후 대조군과 비교하여 개입의 효과를 측정하는 값이며, Mix 2.0 (BiostatXL, Mountain View, CA, USA)로 이용하여 Random effect model을 기준으로 분석하였다. 또한 Grading of Recommen-dations, Assessment, Development and Evaluation (GRADE) 방법론을 사용하여 근거의 확실성을 평가하였다[18]. • 형평성 검토를 위해서 중재의 설계 및 대상자 모집, 결과, 논의 및 제한에 대해 PROGRESS-Plus 프레임워크를 적용하였다[19-21]. PROGRESS-Plus는 연구의 단계에서 고려한 형평성의 요소를 평가하는 것으로, PROGRESS [21]의 요소인 거주지, 인종, 민족, 언어, 문화, 직업, 성별, 종교, 교육, 사회경제적 지위, 사회적 자본, 차별과 관련된 개인의 특성(연령, 장애 등), 관계적 특징(흡연하는 부모의 자녀 등), 시간의 특성(입, 퇴원 등)를 포함하고 있다.
연구 결과
포함된 연구의 특성
포함된 연구의 특성은 Table 1과 같다. 총 15건의 연구 중 RCT 7건, quasi-experimental study는 8건이었다. 15건의 연구 중 6건의 연구는 예방기반 mHealth 중재 효과 평가 연구이며, 9건의 연구는 관리기반 중재를 시행하였다. 연구 대상자 수는 총 1,944명이며, 평균 중재 기간은 10.87주(range: 2-24주)였다. 13건(86.7%)의 연구에서 mHealth 모바일 어플리케이션(앱)을 활용한 중재를 시도하였으며, SNS 활용 1건, 웹을 활용한 연구가 1건이었다. 8건(53.3%)의 연구에서 심혈관 위험인자 또는 비만과 같은 질병상태와 관련하여 대상자를 모집하였으며, 9건 (60.0%)의 연구에서 연구 중재 동안 대상자의 신체활동에 대한 피드백을 제공하였다. 연구의 품질은 RCT의 경우 모두 비뚤림 위험이 낮게 평가되었으며, quasi-experimental study는 낮음에서 심각한 등급으로 평가되었다. 분석에 포함된 논문 중 8건이 학위논문이었으며, 7건이 학술지에 출판된 논문이었다.
Table 1.
Descriptive summary of included studies (K=1,944, n=15)
|
No |
Author (year) |
Type of mHealth |
Sample size |
Participant |
Duration (weeks) |
Intervention |
Comparison |
Design |
QA |
Source |
|
1 |
Kim (2021) [22] |
App |
63 |
Male worker |
12 |
Application of health partnership (home training, provision of medical information, diet) using mobile health apps |
Individual education, booklet provided |
RCT |
Low |
Thesis |
|
2 |
Nam (2017) [23] |
App |
48 |
Operating room nurse |
3 |
Individual exercise using mobile apps |
Booklet provided |
Quasi |
Moderate |
Thesis |
|
3 |
Park (2018) [24] |
SNS |
106 |
Office worker |
12 |
Coaching program for forming exercise habits in daily life using SNS |
Intervention programs with a difference in providing intrinsic rewards |
Quasi |
Serious |
Thesis |
|
4 |
Yang (2021) [25] |
App |
59 |
Smokers among sales service workers |
12 |
Lifestyle improvement program using self-monitoring app (smoking, eating habits, physical activity, drinking) |
Individual health counseling and education |
RCT |
Low |
Thesis |
|
5 |
Yu et al. (2021) [26] |
App |
150 |
Middle-aged (40-69 years old) |
2 |
Use of ‘Dementia Check’ app (dementia management and prevention methods) and brain health trainer (including explanations and videos on dementia prevention exercise methods) |
Everyday life |
RCT |
Low |
Journal |
|
6 |
Yu (2021) [27] |
App |
42 |
Sitting for more than 7 hours a day, complaining of musculoskeletal symptoms |
4 |
Health education, exercise, and health diary writing through mobile apps |
Everyday life |
RCT |
Low |
Thesis |
|
7 |
Lee (2019) [28] |
App, SMS |
48 |
Patients complaining of musculoskeletal symptoms among manufacturing production workers |
8 |
Stretching exercise using a mobile app, providing SMS encouragement |
Providing stretching posters to the workplace |
RCT |
Low |
Thesis |
|
8 |
Choi & Chae (2020) [29] |
App, SMS, Phone, Pedometer |
61 |
Taxi driver |
12 |
Walking exercise using app(daily walking exercise) and pedometer, SMS encouragement text message, phone consultation |
Exercising using self-monitoring apps, walking exercise pamphlets, and pedometers |
Quasi |
Low |
Journal |
|
9 |
Han (2022) [16] |
App |
40 |
Overweight and obese adult female, BMI 23 kg/m2 or more |
12 |
Self-monitoring app, customized personal feedback, online training program (1) MINE group: using online education and self-monitoring applications (2) MINEPlus group: online education, customized personal feedback and self-monitoring application |
Using self-monitoring application |
RCT |
Low |
Thesis |
|
10 |
Kim et al. (2019) [30] |
App |
1,117 |
Metabolic abnormalities |
24 |
Lifestyle monitoring through mobile apps, including online communities, and counseling by physical activity experts |
Individual consultation |
Quasi |
Serious |
Journal |
|
11 |
Park et al. (2017) [31] |
App |
50 |
Young women with low bone density |
20 |
‘Strong bones, Fit body'app (exercise and nutrition records and feedback, health check) and group education |
Everyday life |
RCT |
Low |
Journal |
|
12 |
Kang (2022) [32] |
App |
34 |
Women over 45 years of age, amenorrhea (over 12 months) |
8 |
Exercise guidance using the ‘re-bone’ app |
Providing video contents related to the effectiveness of exercise during menopause |
Quasi |
Serious |
thesis |
|
13 |
Jung & Ha (2019) [33] |
Web, Fitness tracker |
33 |
Production and office workers at chemical manufacturing sites (scale of 150-200 people) |
10 |
Monitoring, counseling and training, and SMS using a fitness tracker (Fitbit) linked with the mobile health portal |
Provide fitness tracker (Fitbit) and self-monitor activity level |
Quasi |
Low |
Journal |
|
14 |
An et al. (2020) [17] |
App |
60 |
Less active group (5000-7499 steps) as an index of physical activity based on a pedometer after performing sedentary office work for more than 5 years. |
12 |
Mobile Healthcare Group (E1): Self-monitoring, exercise-related education, counseling, and feedback using an app (S health) Self-checkup group (E2): self-monitoring of physical activity using an app (SHealth) |
Everyday life |
Quasi |
Serious |
Journal |
|
15 |
Kim et al. (2015) [34] |
App |
33 |
Middle-aged women (subjects with one or more chronic diseases such as hypertension, diabetes, dyslipidemia, and obesity) |
12 |
Combining exercise program and mHealth app (Noom Diet Coach) |
Participation in exercise program |
Quasi |
Low |
Journal |
예방기반 mHealth 중재의 효과
신체활동 증진을 위한 예방기반 mHealth 중재에 대한 결과는 Table 2와 같다. 예방기반 mHealth 중재를 시행한 연구는 6건이었으며, 연구간 결과측정 변수의 차이로 인해 결과변수 중 3가지 변수에 대해서만 통합된 효과크기를 산출하였다. 통합된 효과크기를 산출한 결과 sys-tolic blood pressure (SBP)에 대한 신체활동 증진 프로그램의 효과크기는 2.77 (95% confidence interval, CI: 0.19, 5.34)로 효과크기 해석기준으로 판단했을 때[ 35], 큰 효과크기가 확인되었으나, 중재 후 유의하게 증가함이 확인되었다. diastolic blood pressure (DBP)과 total cholesterol (TC)에 대한 효과는 유의하지 않았다. 이외의 유의한 결과가 확인된 변수 중 중간효과크기를 나타낸 것은 유연성(허리), 운동행위 습관강도, 운동참여 동기, 폐경관련 삶의 질, 일일 걸음수, 체지방률이었다. 결과 변수 중 높은 효과크기를 나타낸 변수는 유연성(다리), 신체활동 자기효능감, 신체활동 행위, 체지방량, 복부지방률, 최대 산소 섭취량이었다. 예방기반 mHealth 중재에 대한 결과 변수의 GRADE 확실성은 낮음에서 높음까지 다양하게 나타났다.
Table 2.
Effectiveness results of prevention-based mobile interventions
|
Outcome and outcome domain |
Author (year) |
Effect estimate (Hedges’ g) |
95% CI |
GRADE certainty |
|
Lower limit |
Upper limit |
|
Systolic blood pressure (SBP) |
Jung & Ha (2019) |
9.94 |
7.29 |
12.59 |
High |
|
An et al. (2020a) |
0.01 |
-0.61 |
0.63 |
Moderate |
|
An et al. (2020b) |
0.28 |
-0.35 |
0.90 |
Moderate |
|
Total |
2.77 (z=2.11) |
0.19 |
5.34 |
|
|
Diastolic blood pressure (DBP) |
An et al. (2020a) |
-8.18 |
-10.40 |
-5.97 |
High |
|
An et al. (2020b) |
0.23 |
-0.39 |
0.85 |
Moderate |
|
An et al. |
-0.65 |
-1.29 |
-0.02 |
Moderate |
|
Total |
-2.49 (z=-1.92) |
-5.03 |
0.05 |
|
|
Triglycerides (TG) |
An et al. (2020a) |
0.00 |
-0.70 |
0.69 |
High |
|
An et al. (2020b) |
-0.27 |
-0.90 |
0.35 |
Moderate |
|
An et al. |
-0.41 |
-1.04 |
0.22 |
Moderate |
|
Total |
-0.24 (z=-1.28) |
-0.62 |
0.13 |
|
|
Flexibility (shoulder, right) |
Nam (2017) |
0.21 |
-0.36 |
0.77 |
High |
|
Flexibility (shoulder, left) |
Nam (2017) |
0.13 |
-0.43 |
0.70 |
High |
|
Flexibility (wrist) |
Nam (2017) |
0.69 |
0.11 |
1.28 |
High |
|
Flexibility (leg) |
Nam (2017) |
0.96 |
0.36 |
1.56 |
High |
|
Number of behavior repetitions |
Park (2018) |
0.22 |
-0.16 |
0.60 |
High |
|
Exercise habit intensity |
Park (2018) |
0.77 |
0.37 |
1.16 |
Low |
|
Exercise participation motivation |
Yu et al. (2021) |
0.75 |
0.42 |
1.08 |
High |
|
Exercise continuation intention |
Yu et al. (2021) |
0.81 |
0.48 |
1.15 |
High |
|
Menopause-specific quality of life (MENQOL) |
Kang (2022) |
-0.74 |
-1.45 |
-0.04 |
High |
|
Handgrip |
Kang (2022) |
-0.30 |
-0.98 |
0.39 |
High |
|
Physical activity self-efficacy |
Jung & Ha (2019) |
2.17 |
1.29 |
3.06 |
High |
|
Physical activity behavior |
Jung & Ha (2019) |
2.25 |
1.35 |
3.15 |
High |
|
Daily walking steps |
Jung & Ha (2019) |
0.75 |
0.03 |
1.47 |
High |
|
Weight |
An et al. (2020a) |
-0.54 |
-1.17 |
0.09 |
Moderate |
|
BMI |
An et al. (2020a) |
-0.32 |
-0.94 |
0.30 |
Moderate |
|
fat mass |
An et al. (2020a) |
-0.88 |
-1.53 |
-0.23 |
High |
|
Body fat (%) |
An et al. (2020a) |
-0.72 |
-1.37 |
-0.08 |
Moderate |
|
Skeletal muscle mass |
An et al. (2020a) |
0.13 |
-0.49 |
0.75 |
Moderate |
|
Waist to Hip ratio (WHR) |
An et al. (2020a) |
-1.23 |
-1.91 |
-0.54 |
High |
|
VO2 max (mL/kg/min) |
An et al. (2020a) |
0.98 |
0.32 |
1.64 |
High |
|
HDL-C |
An et al. (2020a) |
0.35 |
-0.28 |
0.97 |
Moderate |
|
LDL-C |
An et al. (2020a) |
-0.09 |
-0.71 |
0.53 |
Moderate |
|
Fasting blood glucose (FBG) |
An et al. (2020a) |
-0.61 |
-1.25 |
0.03 |
Moderate |
|
Weight |
An et al. (2020b) |
-0.38 |
-1.01 |
0.24 |
Moderate |
|
Body mass index (BMI) |
An et al. (2020b) |
-0.26 |
-0.88 |
0.36 |
Moderate |
|
Fat mass |
An et al. (2020b) |
-0.36 |
-0.98 |
0.27 |
Moderate |
|
Body fat (%) |
An et al. (2020b) |
-0.17 |
-0.79 |
0.45 |
Moderate |
|
Skeletal muscle mass |
An et al. (2020b) |
-0.25 |
-0.87 |
0.37 |
Moderate |
|
Waist to Hip ratio (WHR) |
An et al. (2020b) |
-0.49 |
-1.12 |
0.14 |
Moderate |
|
VO2 max (mL/kg/min) |
An et al. (2020b) |
0.44 |
-0.18 |
1.07 |
Moderate |
|
HDL-C |
An et al. (2020b) |
0.04 |
-0.58 |
0.66 |
Moderate |
|
LDL-C |
An et al. (2020b) |
-0.22 |
-0.85 |
0.40 |
Moderate |
|
Fasting blood glucose (FBG) |
An et al. (2020b) |
-0.33 |
-0.95 |
0.30 |
Moderate |
관리 기반 mHealth 중재의 효과
신체활동 증진을 위한 관리기반 mHealth 중재에 대한 결과는 Table 3과 같다. 관리기반의 mHealth 중재를 제공한 연구는 9건이었으며, 13개의 변수에 대해 통합된 효과크기를 산출하였다. 그 결과 각 변수에 대한 신체활동 증진 프로그램의 효과크기에서 유의한 결과를 나타낸 변수는 운동 자기효능감 1.43 (95% CI: 0.30, 2.57), body mass index (BMI) −0.60 (95% CI: −1.04, −0.17), 복부지방률 −0.48 (95% CI: −0.89, −0.07), 허리둘레 0.34 (95% CI: −0.62, −0.06), 운동 결과기대 1.56 (95% CI: 1.09, 2.03)이었다. 운동 자기효능감과 운동 결과기대는 유의한 향상을 나타냈으며, BMI, 복부지방률, 허리둘레는 유의한 감소가 확인되었다. 이외 통합된 효과크기를 산출한 결과변수 중 fasting blood sugar (FBS), TC, triglycerides (TG), high density lipoprotein (HDL), SBP, DBP, 건강관련 삶의 질, 체중, 신체활동에서는 유의한 결과가 나타나지 않았다. 이외 변수 중 유의한 결과를 나타낸 변수는 악력(좌, 우), 다리근력, 내장지방 변화, 건강관리 자기효능감, 걷기, 운동이익, 운동만족감(정신, 신체), 생활습관 관련 건강행위(운동), 건강증진 행위(HPLP-II) 중 신체활동이었다. 관리기반 mHealth 중재에 대한 결과 변수의 GRADE 확실성은 중등도에서 높음까지 다소 높게 나타났다.
Table 3.
Effectiveness results of management-based mobile interventions
|
Outcome and outcome domain |
Author (year) |
Effect estimate (Hedges’ g) |
95% CI |
GRADE certainty |
|
Lower limit |
Upper limit |
|
Self-efficacy in exercise |
Kim (2021) |
1.29 |
0.74 |
1.84 |
High |
|
Yang (2021) |
4.48 |
3.50 |
5.46 |
High |
|
Lee (2019) |
-0.01 |
-0.58 |
0.56 |
High |
|
Choi & Chae (2020) |
1.38 |
0.82 |
1.94 |
High |
|
Park et al. (2017) |
0.31 |
-0.25 |
0.87 |
High |
|
Total |
1.43 (z=2.47) |
0.30 |
2.57 |
|
|
Body mass index (BMI) |
Kim (2021) |
-0.41 |
-0.91 |
0.09 |
High |
|
Yang (2021) |
-1.34 |
-1.91 |
-0.77 |
High |
|
Choi & Chae (2020) |
0.07 |
-0.43 |
0.58 |
Moderate |
|
Han (2022a) |
-0.65 |
-1.29 |
-0.01 |
High |
|
Han (2022b) |
-1.08 |
-1.75 |
-0.41 |
High |
|
Kim et al. (2015) |
-0.29 |
-0.98 |
0.40 |
High |
|
Total |
-0.60 (z=-2.70) |
-1.04 |
-0.17 |
|
|
Waist to Hip Ratio (WHR) |
Kim (2021) |
-0.56 |
-1.06 |
-0.05 |
High |
|
Kim et al. (2015) |
-0.33 |
-1.02 |
0.36 |
High |
|
Total |
-0.48 (z=-2.31) |
-0.89 |
-0.07 |
|
|
Fasting blood sugar (FBS) |
Kim (2021) |
-1.09 |
-1.62 |
-0.56 |
High |
|
Yang (2021) |
0.98 |
0.43 |
1.52 |
High |
|
Kim et al. (2015) |
0.22 |
-0.46 |
0.91 |
High |
|
Total |
0.03 (z=0.05) |
-1.24 |
1.31 |
|
|
Total cholesterol (TC) |
Kim (2021) |
-0.71 |
-1.22 |
-0.20 |
High |
|
Yang (2021) |
-0.09 |
-0.60 |
0.42 |
High |
|
Kim et al. (2015) |
-0.09 |
-0.77 |
0.59 |
High |
|
Total |
-0.32 (z=-1.47) |
-0.74 |
0.11 |
|
|
Triglycerides (TG) |
Kim (2021) |
-1.02 |
-1.55 |
-0.50 |
High |
|
Kim et al. (2015) |
-0.13 |
-0.81 |
0.56 |
High |
|
Total |
-0.60 (z=-1.35) |
-1.48 |
0.28 |
|
|
HDL-C |
Kim (2021) |
0.69 |
0.18 |
1.20 |
High |
|
Kim et al. (2015) |
-0.49 |
-1.19 |
0.20 |
High |
|
Total |
0.12 (z=0.21) |
-1.03 |
1.28 |
|
|
Waist circumference (WC) |
Yang (2021) |
-0.17 |
-0.68 |
0.35 |
High |
|
Choi & Chae (2020) |
-0.25 |
-0.75 |
0.26 |
Moderate |
|
Han (2022a) |
-0.41 |
-1.04 |
0.22 |
High |
|
Han (2022b) |
-0.68 |
-1.32 |
-0.04 |
High |
|
Total |
-0.34 (z=-2.37) |
-0.62 |
-0.06 |
|
|
Systolic blood pressure (SBP) |
Yang (2021) |
-2.06 |
-2.70 |
-1.42 |
High |
|
Choi & Chae (2020) |
-0.53 |
-1.04 |
-0.02 |
Moderate |
|
Han (2022a) |
0.28 |
-0.35 |
0.90 |
High |
|
Han (2022b) |
0.34 |
-0.28 |
0.97 |
High |
|
Kim et al. (2015) |
-0.56 |
-1.26 |
0.14 |
High |
|
Total |
-0.50 (z=-1.20) |
-1.33 |
0.32 |
|
|
Diastolic blood pressure (DBP) |
Yang (2021) |
-0.60 |
-1.13 |
-0.08 |
High |
|
Choi & Chae (2020) |
-0.74 |
-1.26 |
-0.22 |
Moderate |
|
Han (2022a) |
0.72 |
0.08 |
1.36 |
High |
|
Han (2022b) |
0.83 |
0.18 |
1.48 |
High |
|
Kim et al. (2015) |
-0.46 |
-1.15 |
0.24 |
High |
|
Total |
-0.06 (z=-0.19) |
-0.72 |
0.60 |
|
|
Health-related QoL |
Choi & Chae (2020) |
1.65 |
1.07 |
2.24 |
High |
|
Han (2022a) |
0.26 |
-0.37 |
0.88 |
High |
|
Han (2022b) |
0.20 |
-0.42 |
0.82 |
High |
|
Total |
0.71 (z=1.46) |
-0.24 |
1.66 |
|
|
Weight |
Han (2022a) |
-0.41 |
-1.04 |
0.21 |
High |
|
Han (2022b) |
0.14 |
-0.48 |
0.77 |
High |
|
Kim et al. (2015) |
-0.18 |
-0.86 |
0.51 |
High |
|
Total |
-0.14 (z=-0.76) |
-0.52 |
0.23 |
|
|
Outcome expectation for exercise |
Choi & Chae (2020) |
1.66 |
1.08 |
2.25 |
Moderate |
|
Kim et al. (2015) |
1.38 |
0.61 |
2.15 |
High |
|
Total |
1.56 (z=6.54) |
1.09 |
2.03 |
|
|
Physical activity |
Yu (2021) |
0.96 |
0.32 |
1.60 |
High |
|
Han (2022a) |
-5.16 |
-6.50 |
-3.81 |
High |
|
Han (2022b) |
2.29 |
1.48 |
3.11 |
High |
|
Kim et al. (2019) |
6.86 |
6.54 |
7.18 |
Moderate |
|
Total |
1.27 (z=0.56) |
-3.15 |
5.70 |
|
|
Musculoskelectal symptom (neck) |
Lee (2019) |
0.22 |
-0.35 |
0.79 |
High |
|
Musculoskelectal symptom (shoulder) |
Lee (2019) |
0.38 |
-0.19 |
0.96 |
High |
|
Musculoskelectal symptom (back) |
Lee (2019) |
-0.19 |
-0.76 |
0.38 |
High |
|
Musculoskelectal symptom (hands/wrist) |
Lee (2019) |
-0.11 |
-0.68 |
0.46 |
High |
|
Musculoskelectal symptom (arms) |
Lee (2019) |
0.09 |
-0.48 |
0.65 |
High |
|
Musculoskelectal symptom (legs) |
Lee (2019) |
-0.10 |
-0.66 |
0.47 |
High |
|
Musculoskelectal symptom (feet/ankles) |
Lee (2019) |
-0.39 |
-0.97 |
0.18 |
High |
|
Social support in exercise |
Lee (2019) |
0.37 |
-0.21 |
0.94 |
High |
|
Physical fitness (flexibility, back [sit-down]) |
Lee (2019) |
0.03 |
-0.53 |
0.60 |
High |
|
Grip power (Lt.) |
Lee (2019) |
-0.74 |
-1.33 |
-0.15 |
High |
|
Grip power (Rt.) |
Lee (2019) |
-0.67 |
-1.25 |
-0.08 |
High |
|
Leg strength |
Lee (2019) |
-0.69 |
-1.28 |
-0.11 |
High |
|
Abdominal strength |
Lee (2019) |
-0.18 |
-0.74 |
0.39 |
High |
|
Performing stretching exercises |
Lee (2019) |
-0.28 |
-0.86 |
0.29 |
High |
|
Fat Changes (%) |
Han (2022a) |
-0.29 |
-0.91 |
0.33 |
High |
|
VFA Changes (cm2) |
Han (2022a) |
-0.47 |
-1.10 |
0.16 |
High |
|
Body shape satisfaction (BSQ changes) |
Han (2022a) |
-0.45 |
-1.08 |
0.18 |
High |
|
Self-efficacy in health management (KSRAPH changes) |
Han (2022a) |
0.45 |
-0.18 |
1.07 |
High |
|
Fat Changes (%) |
Han (2022b) |
-0.48 |
-1.11 |
0.15 |
High |
|
VFA Changes (cm2) |
Han (2022b) |
-0.76 |
-1.41 |
-0.12 |
High |
|
Body shape satisfaction (BSQ changes) |
Han (2022b) |
-0.56 |
-1.20 |
0.07 |
High |
|
Self-efficacy in health management (KSRAPH changes) |
Han (2022b) |
0.68 |
0.04 |
1.32 |
High |
|
Walking (Subdomains of health behaviors) |
Kim et al. (2019) |
7.76 |
7.40 |
8.11 |
Low |
|
Benefits of exercise |
Park et al. (2017) |
0.71 |
0.13 |
1.28 |
High |
|
Barriers of exercise |
Park et al. (2017) |
-0.57 |
-1.14 |
0.00 |
High |
|
Exercise adherence (enabling) |
Kim et al. (2015) |
-0.13 |
-0.81 |
0.56 |
High |
|
Exercise adherence (reinforcing) |
Kim et al. (2015) |
-0.16 |
-0.84 |
0.52 |
High |
|
Exercise adherence (predisposing) |
Kim et al. (2015) |
0.69 |
-0.02 |
1.39 |
High |
|
Exercise satisfaction (psychological) |
Kim et al. (2015) |
0.47 |
-0.23 |
1.16 |
High |
|
Exercise satisfaction (mental) |
Kim et al. (2015) |
1.41 |
0.64 |
2.18 |
High |
|
Exercise satisfaction (physical) |
Kim et al. (2015) |
0.86 |
0.14 |
1.57 |
High |
|
Exercise satisfaction (interpersonal relationship enhancement) |
Kim et al. (2015) |
0.02 |
-0.66 |
0.71 |
High |
|
Fat (%) |
Kim et al. (2015) |
-0.33 |
-1.02 |
0.36 |
High |
|
Fat (kg) |
Kim et al. (2015) |
-0.27 |
-0.95 |
0.42 |
High |
|
LDL-C |
Kim et al. (2015) |
0.15 |
-0.54 |
0.83 |
High |
|
Lifestyle related health behavior (exercise) |
Yang (2021) |
2.31 |
1.64 |
2.98 |
High |
|
Physical activity among health-promoting behaviors (HPLP-II) |
Yu (2021) |
1.51 |
0.82 |
2.21 |
High |
건강불평등에 영향을 미치는 요인에 대한 고려
체계적 문헌고찰에 포함된 연구의 mHealth 중재 설계 및 연구 참여자 모집, 연구 결과, 논의 또는 연구의 제한점에서 PROGRESS-Plus 프레임워크에 나열된 요소를 포함하거나 고려한 연구에 대한 검토를 시행하였다( Figure 2).
Figure 2.
Number of studies considering the PROGRESS-Plus factors. 
중재설계 및 대상자 모집의 PROGRESS-Plus 요인 보고
중재설계 및 대상자 모집의 단계에서 연구의 73.3% (11/15)에서 하나 이상의 PROGRESS-Plus 요인을 고려하였다. 중재 설계에서 Yang [ 25]의 연구에서는 연구 대상자의 연령을 고려하여 앱을 간결한 문장과 단순한 기능으로 설계하였으며, Lee [ 28]는 균형유지에 어려움이 있는 동작을 제외하였다. Kang [ 32]은 폐경기 여성의 과도한 운동은 건강에 악영향을 줄 수 있어 운동시스템을 하루 1번만 사용할 수 있도록 제한하였으며, 특정 연령층을 대상으로 설계된 연구가 3건 있었다[ 26, 32, 33]. 또한 특정 성별로 연구 참여자를 제한한 연구가 6건[ 26, 29, 31- 34]이었다. 성별에 대한 고려는 특정 성별의 고유한 요구를 해결하기 위해 중재를 맞춤화하는 방법으로 고려되었으며[ 16, 17, 22, 31, 32, 34], 남성을 대상으로 수행된 연구가 1건[ 22] 여성을 위한 연구가 5건이었다[ 16, 17, 31, 32, 34]. 직업에 대한 고려로는 직업의 특성상 앉아있는 시간이 상대적으로 긴 사무직과 택시운전자를 위해 수행한 연구가 2건[ 17, 29]이었으며, 근골격계 증상 호소가 많은 의료인 중에서도 수술실 간호사를 위한 근골격계증상 개선을 시도한 연구가 1건 있었다[ 23]. 직업적 특성에 사회적 자본을 고려한 연구로는 보건관리자가 상주하지 않아 보건교육의 기회나 예방관련 활동이 취약한 소규모 사업장을 대상으로 수행한 연구가 3건[ 22, 26, 33] 있었으며, 그중 Lee [ 28]의 연구는 산업재해와 근골격계 질환 발생률이 높은 제조업 생산직 근로자를 대상으로 연구가 수행되었으며, 사업장의 환경을 고려하여 의자나 벽을 이용한 동작 등 시설이나 공간에 제약을 받는 동작은 제외하였다. 또한, 2건의 연구에서 온라인을 통해 연구 대상자를 모집하여 다양한 거주지, 직업을 가진 대상자가 모집될 수 있도록 하였다[ 27, 32]. 사회경제적 상태에 대한 고려로는 Yu [ 27]의 연구에서 앱 구독비용을 연구자가 지불하여 개인이 비용의 부담없이 연구에 참여할 수 있도록 하였으며, 중재에 활용될 기기(스마트밴드, 만보기, 혈압계, 혈당계, 체성분 측정장치) 등을 제공한 연구가 4건 있었다[ 26, 29, 30, 33]. 개인의 특성에 대한 고려는 연구 대상자 선정 및 제외기준에 주로 포함되었다[ 16, 17, 22, 25, 27- 31, 33, 34]. 선정기준에서 신체활동량이 적은 대상자를 대상으로한 연구가 1건[ 17], 질병 상태나 위험에 대한 고려로 만성 질환을 가진 자에 대한 연구 3건[ 22, 29, 34] 심혈관질환 위험인자를 가진 자 2건[ 22, 25], 근골격계 증상 호소자 2건[ 27, 28], 과체중 또는 비만인 대상자 2건[ 16, 34], 대사 이상 유소견자[ 30]와 골밀도가 낮은 자[ 31]를 대상으로 한 연구가 있었다. 또한 신체활동 증진 중재의 효과를 평가하기 위해 신체활동량이 많은 경우 1건[ 33], 이미 규칙적으로 운동을 시행하거나 다른 관리 프로그램에 참여하는 환자를 제외한 연구가 5건[ 16, 25, 27- 29]있었다. 중재 설계나 대상자 모집에서 인종, 민족, 문화, 언어, 종교, 교육과 관계적 특징이나 시간의 특성에 대해 보고한 연구는 없었다.
연구 결과에서 PROGRESS-Plus 요인 보고
체계적 문헌고찰에 포함된 모든 연구는 결과에서 PROGRESS-Plus 요소를 설명하였으며, 주로 연구참여자의 인구학적 특성에 대한 통계의 일부로 보고되었다. 인구학적 특성 중 주로 보고된 특성은 연령[ 16, 17, 22, 24- 33], 성별[ 23- 28, 30], 교육[ 26, 27, 29, 30, 33], 결혼[ 22, 28, 33], 직업[ 17, 22, 23, 25- 28, 33], 사회경제적 상태[ 27, 29, 31]였다. 이 외 개인특성에 대해서는 질환[ 16, 22, 24, 29, 31], 운동과 신체활동 정도[ 23- 25, 27, 30], 가족력[ 25, 29], 흡연[ 25, 27, 29, 30], 음주[ 27, 29, 30], 식습관[ 30, 31]이 보고되었다. 또한 mHealth 중재와 관련된 개인의 특성(mHealth 활용경험, mHealth 앱의 활용인식, mHealth 앱의 활용 선호도, 디지털 문해력 등)이 3건의 연구에서 보고되었다[ 22, 26, 29]. 결과에서 인종, 민족, 문화, 언어, 종교, 사회적 자본, 관계적 특징이나 시간의 특성에 대해 보고한 연구는 없었다.
논의 또는 연구의 제한점에서 PROGRESS-Plus 요인 보고
본 체계적 문헌고찰에 포함된 연구 중 93.3% (14/15)의 연구에서 논의 또는 제한에서 PROGRESS-Plus 요인을 보고하였다. 가장 많이 언급된 PROGRESS-Plus 요인으로는 소규모 사업장의 전문적 건강관리를 위해 전임 보건관리자 배치를 위한 제도적 개선의 필요성 등을 언급한 사회적 자본 5건[ 22, 24- 27, 32], mHealth 서비스 제공시 고령 참여자가 직면하는 앱 사용의 문제와 같은 연령의 요소를 보고한 연구 4건[ 22, 23, 33, 34], 사회경제적 요소에 대해서 소규모 사업장의 건강증진 사업 시행의 미흡한 실태 등을 보고한 연구가 4건 있었다[ 25, 28, 32, 33]. 기타 요인으로 연구참여자 개인특성 중 연구 대상자의 다양성 부족에 대해 2건의 연구에서 보고되었으며[ 23, 30], 모바일 앱 활용능력의 차이에 대한 고려가 1건의 연구에서 보고되었다. 이외 거주지[ 29], 교육[ 16], 성별[ 30], 직업[ 29]에 대한 요인이 보고되었고, PROGRESS-Plus 요인이 한 가지만 보고된 연구가 5건[ 16, 23, 24, 28, 29], 두 가지 이상 보고된 연구가 9건이었다[ 22, 25- 27, 30- 34]. 논의 및 연구의 제한점에서 인종, 민족 문화, 언어, 종교, 관계적 특징이나 시간의 특성에 대해 보고한 연구는 없었다.
고 찰
본 체계적 검토는 한국 성인을 대상으로 수행된 mHealth 서비스를 이용한 신체활동 증진 중재의 질병 예방 및 건강관리 효과를 검토하고, PROGRESS-Plus 프레임워크를 사용하여 중재의 설계, 시행, 결과평가에서 건강 및 사회적 형평성 요인의 고려 여부를 확인하였다. 한국 성인의 신체활동 증진을 목표로 하는 mHealth 서비스는 다양한 변수의 결과를 통해 신체 활동량 증진, 건강지표의 개선, 신체활동과 관련된 주관적 지표 개선에 긍정적 효과가 확인되었다. 이는 mHealth 서비스 제공시 대면서비스에 비해 더욱 빈번하고 지속적으로 서비스 제공이 가능한 특성으로 인한 결과라고 판단해 볼 수 있다[ 36]. 본 검토에 포함된 연구 중 86.7%의 연구가 mHealth 앱을 활용하여 중재를 제공하여, 선행 연구에서 모바일 앱이 건강행동 변화에 유용한 도구로 확인되었으며[ 37], 신체활동 개선을 통해 비전염성 질병 예방에 효과적이라는 것과 같은 결과라 할 수 있다[ 38]. 또한 9건(60%)의 연구에서 개인 맞춤 피드백을 제공하였으며, 자가 모니터링을 시행한 연구도 7건(46.7%)이었다. 개인 맞춤 피드백은 다양한 참여자를 수용할 수 있는 중요한 방법으로[ 39], 신체활동 앱을 통한 자가 점검 및 개인맞춤 피드백을 제공하는 경우, short message service (SMS)를 통하여 격려나 관련 정보를 제공받은 그룹과 앱을 활용하여 자가점검만을 시행한 그룹보다 더 장기간 신체 활동량이 유의하게 증가되는 것을 확인한 Han and Suh [ 40]의 연구와 일치하는 결과이다. 연구 간의 이질성으로 결과변수 중 예방기반 중재에서 3가지 변수와 관리기반 중재에서 13가지의 변수에서 통합된 효과크기를 산출하였다. 그 결과 예방기반 중재에서는 SBP이 유의한 효과가 나타났으나, 유의한 증가가 확인되었다. 이는 건강개선지표로는 적절치 않으나, 예방기반 신체활동 중재에 포함된 6건의 연구 대상자는 모두 건강한 대상자로 정상범위 혈압을 유지하는 대상자일 가능성이 높아 이러한 결과를 나타냈다고 판단할 수 있다. 이는 신체활동 증진 중재를 제공하고 혈압에서 유의한 결과가 나타나지 않은 선행연구 결과와 일부 일치하는 결과라고 판단할 수 있다[ 41, 42]. 관리기반 중재에서는 운동자기 효능감과 운동결과 기대의 유의한 향상, BMI, 복부지방률, 허리둘레는 유의한 감소로 객관적, 주관적 지표에서 유의한 값이 확인되었다. 관리기반 중재가 유의한 결과를 나타낸 것은 관리기반 중재에 포함된 모든 연구는 질병 유소견자 및 만성질환자들을 대상으로 하여, 운동과 같은 건강관리의 요구도 및 실천도가 건강한 대상자보다 높았음을 짐작해 볼 수 있다. 예방기반 중재는 약 66.6% (4건)의 연구만이 앱과 다른 중재를 병행하였으나, 관리기반 중재는 모든 연구에서 앱을 포함하여 교육, 상담, SMS, 모니터링, 그룹교육 등 하나 이상의 중재를 동시에 시도하여, 모바일 앱 중재에 다른 중재 전략을 함께 사용할 경우 앱만을 사용할 경우보다 더 크고 지속되는 효과를 가져올 수 있다는 선행연구 결과와 일치하는 결과를 보였다[ 38]. 하지만, 도구를 통해 평가된 결과의 경우 주관적 평가로 과다 평가의 가능성이 있으며, 직접적인 신체활동 증진의 결과를 나타내는 결과변수가 아니므로 해석에 주의가 필요하다. 이와 함께 신체활동량 증진의 지표로 검사실 결과를 확인하였지만, 이는 다른 영향을 통제할 수 없어 신체활동 개선의 결과만을 반영했다고 할 수 없다. 분석에 포함된 모든 연구는 대상자의 특성을 제시할 때 PROGRESS-Plus 요인을 보고하였다. 이는 연구가 다양한 대상자에 대해 적합성 여부를 결정하기 위한 의도적 접근방식이 아니라, 연구 참여자의 인구학적 특성을 보고하는 연구 관행의 일부였다. 분석에 포함된 15편의 중재에 대한 PROGRESS-Plus 요인의 검토 결과 거주지, 직업, 성별, 교육, 사회경제적 상태, 사회적 자본, 개인의 특성(신체활동, 질병, 결혼, 음주나 흡연, mHealth 관련 특성) 등이 고려되었음이 확인되었다. 거주지에 대한 고려는 Yu [ 27]와 Kang [ 32]의 연구에서 각각 온라인 광고와 온라인 커뮤니티를 이용하여 연구 참여자를 모집하여, 거주지에 제한을 두지 않은 모집방식을 통하여 이루어졌으며, 이는 직업과 개인의 특성에 대한 형평성도 고려한 모집방식이라고 할 수 있다. 성별에 대한 고려는 중재 설계의 단계에서 특정 성별의 고유한 요구를 해결하기 위해 중재를 맞춤화하는 방식으로 고려되었다. 성별의 차이는 질병의 위험, 발병률, 의료서비스의 필요성과 같이 건강에 다양한 영향을 미치는 요인으로[ 21], 본 연구에서는 남성 대상 연구 1건(심혈관 위험인자 자가관리 중재), 여성 대상 연구 5건(체중관리, 뼈건강 향상, 폐경기 신체활동 증진) 수행되었다. 특히 한국 기혼 여성의 경우 배우자와 자녀 양육의 역할과 책임, 상대적으로 낮은 사회적 지위로 인해 건강관리를 소홀히 하거나, 건강을 위해 가용한 자원이 제한될 수 있어 이에 대한 고려가 필요할 것이다[ 43]. 직업에 대한 고려로는 업무 양상에 따른 건강위험을 관리하기 위한 중재가 2건 확인되었다. 장시간 좌식 업무를 하는 택시 운전자, 근골격계 증상 호소가 많은 의료인을 대상으로 연구가 수행되었으며, 이외에도 사무직 근로자, 생산직 근로자를 대상으로 한 연구가 확인되었다. 교육의 경우 Han [ 16]의 연구 참여 대상자가 일 대학의 구성원인 고학력 참여자로 이루어져, 연구 결과의 일반화가 제한된다는 제한점을 제시하였고, 이외 연구의 경우 인구학적 통계에는 보고되었지만, 중재의 설계나 대상자 모집에 고려되지 않았다. 교육 수준이나 개인의 특성 중 mHealth의 이용과 관련하여, 문해력의 수준이 낮을 경우 자신에게 적절하고 이용가능한 mHealth 서비스를 찾는 능력이나 이용에 어려움이 있을 수 있다[ 44]. 이는 건강에 직접적 영향이 있다는 것보다, 건강에 영향을 미치는 변수들(건강지식, 건강행동, 자기관리 등)에 영향을 주게 되므로[ 45], 대상자의 특성에 따라 중재의 설계 및 시행에 이에 대한 고려가 필요할 것이다. 사회경제적 상태에 대한 고려로는 인구통계학적 통계에 대한 보고 외, 중재 시행 시 앱 구독 비용 지원 1건, 중재에 활용되는 장비를 지원한 연구가 4건 있었으며, 연구의 제한점으로 소규모 사업장의 건강증진 사업 시행이 미흡한 실태를 보고한 연구가 4건 있었다. 점차 다양한 디지털 장비가 mHealth 에 활용되고 있으며, 소득과 교육수준이 높은 경우 이러한 장비를 소유하고 있는 비율이 높다[ 44]. 비용지출은 기술사용에 대한 일반적 장벽으로 보고되고 있으며, 최근 이를 치료에 활용하는 디지털 치료제의 등장으로 추후 연구에서는 사회경제적 상태에 대한 고려가 더욱 필요할 것이라 사료된다[ 46]. 사회적 자본은 연구설계에서 보건관리자가 상주하지 않아 보건관리에 취약한 소규모 사업장 대상 연구 3건, 직장환경을 고려한 운동 동작을 프로그램에 반영한 연구 1건 있었다. 이와 함께, 논의를 통해 소규모 사업장의 건강관리를 위한 전임 보건관리자의 배치를 위해 제도 개선의 필요성 등을 언급한 연구가 5건 있었다. PROGRESS-Plus 요인 중 차별을 유발할 수 있는 개인의 특성으로는 연령이 가장 많이 고려된 요인이었다. 연구 설계에서 특정 연령층을 대상으로 설계된 연구 3건이었으며, 연령을 고려하여 앱을 설계하거나 프로그램을 설계한 연구가 3건 있었다. 여성과 젊은 연령층이 고령층에 비해 모바일 앱의 사용에 더 능숙한 경향이 있어[ 47, 48], 연구의 제한점에서 mHealth 서비스 제공 시 고령 참여자의 앱 사용의 문제를 보고한 연구가 있었다. 이외 개인 특성 중 질병, 결혼, 기호식품(흡연, 음주) 등이 연구에서 형평성에 관련한 고려 요인으로 확인되었다. 형평성에 대한 고려 요인은 연구 참여자의 인구학적 특성 결과를 제외하면 대부분 중재 설계에서 고려되었으며, 논의와 연구의 제한점에서 연구의 한계나 추후 연구의 확장성을 제시하는데 반영되었다. 하지만 PROGRESS-Plus 요인 중 인종, 민족, 문화, 언어, 종교, 관계적 특징이나 시간의 특성을 고려한 연구는 없었다. 2022년 말 기준으로 국내 체류 외국인은 약 220만 명이며 전년대비 14.8% 증가한 추세로[ 49], 추후 연구에서는 국내 외국인 비율을 고려하여 인종, 민족, 문화, 언어, 종교의 특성을 반영한 연구의 수행을 고려해 볼 수 있을 것이다. 본 검토는 PROGRESS-Plus 형평성 프레임워크를 활용하여 한국 성인을 위한 신체활동 증진 중재에 대한 최상의 증거를 확인하기 위해 개념화되고 설계되었다. 문헌검색, 데이터 추출, 연구의 품질 평가는 한국보건의료연구원의 매뉴얼과 Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 기반으로 연구자 2인의 동의하에 이중으로 검토되었으며, 프로토콜을 공개하여 재현 가능하도록 하였다. 선정된 연구에서 데이터를 추출하고 각 결과를 RoB, Risk of Bias In Non-randomized Study of Interventions (ROBINS-I)를 활용하여 비판적으로 평가하였으며, GRADE 방법론을 활용하여 증거의 확실성에 대한 평가를 수행하였다. 또한, 이 연구는 우리가 아는 한 형평성 렌즈를 적용하고, 한국 성인의 mHealth 중재의 건강 형평성의 영향을 탐색한 최초의 체계적 문헌고찰이라는 것에 연구의 의의가 있다.
본 연구의 제한점으로는 데이터 검색이 한국보건의료연구원에서 권장하는 COre database를 중심으로 수행되었지만, 이외 DB를 반영하지 않아 재현성에 영향을 미칠 수 있다. 또한 동료검토를 거치지 않은 학위논문이 분석에 포함된 15건의 연구 중 8건으로 연구결과 확장에 주의가 필요할 것이다. 추후 연구에서는 본 연구에서 제외한 단일군 연구를 포함한 검토가 필요할 것이며, 본 연구에서 정량적 연구 결과만으로 건강 형평성에 영향을 줄 수 있는 특성을 확인하였다면, 이후 연구에서는 정성적 연구를 포함하여 연구 결과를 보완할 필요가 있을 것이다. 각 중재에서 프로그램 참여에 대한 효과가 일치하는 부분도 있지만 상이한 결과를 나타내는 부분도 있어, 보다 객관적인 측면에서 통합하고 이를 활용하기 위한 메타분석 연구를 수행할 필요성을 제기한다.
결 론
본 연구는 최근 10년 동안 국내 성인을 대상으로 신체활동 증진을 위해 시행된 예방과 관리기반 mHealth 중재들을 조사하고, 그 효과와 건강 형평성 중심의 검토를 위해 시행되었다. 신체활동 증진을 위한 mHealth 중재의 검토 결과, 다양한 변수의 개선을 통해 긍정적 효과를 확인하였다. 또한, 각 연구에 대해 PROGRESS-Plus 형평성 프레임워크를 활용한 검토하여 국내 성인을 위한 신체활동 증진 mHealth 중재에서 중요하게 고려된 형평성 요소를 확인하였으며, 인종, 민족, 문화, 언어, 종교 등 향후 연구에서 추가로 고려가 필요한 영역에 대해 확인한 것에 연구의 의의가 있다고 할 수 있다.
REFERENCES
2. Powers SK, Dodd SL, Jackson EM. Total fitness & wellness.. 6th ed.. Boston: Pearson; 2014.
3. Kelley GA, Kelley KS. Effects of aerobic exercise on C-reactive protein, body composition and VO2max in adults? a meta-analysis of randomized controlled trials. Metabolism 2006;55(11):1500-1507. DOI: 10. 1016/j.metabol.2006.06.021.   4. Penedo FJ, Dahn JR. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry 2005;18(2):189-193. DOI: 10.1097/00001504-200503000-00013. 6. Varshney U. Pervasive healthcare computing: EMR/EHR, wireless and health monitoring. New York: Springer; 2009.
9. Finkelstein J, Bedra M, Li X, Wood J, Ouyang P. Mobile app to reduce inactivity in sedentary overweight women. Stud Health Technol Inform 2015;216:89-92. 11. Korea Health Promotion Institute. National health plan Available at https://www.khepi.or.kr/ [accessed on April 10, 2023]. 13. Kim H. ‘Health equity’ goals in the 5th National Health Plan (HP2030): Based on the evaluation of Health Plan 2020 and international cases studies. Korean J Health Educ Prom 2021;38(4):33-51. (Korean).DOI: 10.14367/kjhep.2021.38.4.33. 14. Choi IS, Kim HS, Hwang SH, Kim HW, Noh YM. National evidence-based healthcare collaborating agency (NECA). Seoul: National Evi-dence-based Healthcare Collaborating Agency; 2011. (Korean).
15. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updatedguideline for reporting systematic reviews. Int J Surg 2021;88:105906. DOI: 10.1016/ j.ijsu.2021.105906. 16. Han YM. Effect of an online weight management education program on weight and psychological factors for overweight and obese women [dissertation] Seoul National University; Korea: 2022.
17. An JH, Lee YM, Choi S. The effects of physical activity intervention in mobile healthcare on obesity, cardiorespiratory fitness, metabolic syndrome risk factors. Korean Soc Sports Sci 2020;29(3):795-806. (Korean).DOI: 10.35159/kjss.2020.06.29.3.795. 18. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozeket J, et al. GRADE guidelines: 1. Introduction— GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 2011;64(4):383-394. DOI: 10.1016/ j.jclinepi.2010.04.026. 19. Oliver S, Dickson K, Newman M. Getting started with a review. An introduction to systematic reviews. London: SAGE Publications; 2012.
20. Oliver S, Kavanagh J, Caird J, Lorenc T, Oliver K, Harden A, et al. Health promotion, inequalities and young people's health: A systematic review of research. London: EPPI-Centre; 2008.
21. O’ Neill J, Tabish H, Welch V, Petticrew M, Pottie K, Clarke M, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol 2014;67(1):56-64. DOI: 10.1016/j.jclinepi.2013. 08.005. 22. Kim EJ. Effects of a health partnership using mobile health application for male workers with cardiovascular risk factors in small and medium enterprises [dissertation] Hanyang University; Korea: 2021.
23. Nam HW. Development and evaluation app-based musculoskeletal exercise program (AMSEP) for nurses in operating rRoom [dissertation] Keimyung University: Korea; 2017.
24. Park MH. Development of SNS platform based healthy lifestyle coaching program and effectiveness evaluation [dissertation] Seoul National University; Korea: 2018.
25. Yang HK. Development and effect of lifestyle improvement program using self-monitoring app to reduce risk factors for cardio-cerebrovas-cular disease [dissertation] Kyung Hee University; Korea: 2021.
26. Yu HS, Hwang IS, Park HJ. An empirical study on usage effect of dementia prevention mobile application. J Korean Soc Wellness 2021;16(3):1-8. (Korean).DOI: 10.21097/ksw.2021.08.16.3.1. 27. Yu HJ. Effect of the use of a mobile health application for musculoskeletal symptom management on self-management [dissertation] Sah-myook University; Korea: 2021.
28. Lee RS. Comparison of effects of app-based stretching exercise programs on musculoskelectal symptoms of small company workers [dissertation] Chonnam National University; Korea: 2019.
31. Park YJ, Lee SJ, Shin NM, Shin H, Jeon S, Lee J, et al. Application and effect of mobile type-bone health intervention in Korean young adult women with low bone mass: A randomized control trial. Asian Nurs Res 2017;11(1):56-64. (Korean).DOI: 10.1016/j.anr.2017.03.005. 32. Kang HM. Design and validation of digital healthcare service ‘Re-bone’ for menopause women [dissertation] Yonsei University; Korea: 2022.
33. Jung M, Ha Y. Effectiveness of a workplace walking program using a fitness tracker including individual counseling and tailored text mes-saging. J Korean Acad Community Health Nurs 2019;30(3):257-270. (Korean).DOI: 10.12799/jkachn.2019.30.3.257.  34. Kim TU, Kim SC, Cho EH. The effects of using m-Health app to the body composition, blood and related variable of exercise adherence of mMiddle-aged obese female. Korean J Phys Educ 2015;54(2):407-419. (Korean).
35. Cohed J. A power primer. Psychol Bull 1992;112(1):155-159. DOI: 10. 1037//0033-2909.112.1.155. 40. Han A, Suh S. Effects of mobile healthcare application use and SMS/MMS as physical activity intervention on the levels of physical activity. J Leis Stud 2017;15(2):39-59. (Korean).
43. Jeon GS, Choi ES, Lee HY. Gender-related difference in the utilization of health care services by Korean adults. J Korean Pubilc Health Nurs 2010;24(2):182-196. (Korean).DOI: 10.5932/JKPHN.2010.24.2.182.
45. Kim J. Meta analysis of the correlation between health literacy and health related variables. Korean J Health Educ Prom 2018;5(1):101-113. (Korean).DOI: 10.14367/kjhep.2018.35.1.101. 46. Min SD. Evolution of healthcare solutions according to environmental changes. KIEE Magazine 2023;72(3):16-21. (Korean).
|
|